
Cracked Tooth Revival
Amalgam (silver) fillings are self-setting alloy restorations that are packed and locked into the tooth with mechanical retention. Though these restorations can survive up to thirty years in service, the sharp, box-like preparations and undercuts required to retain the alloy often lead to catastrophic fractures. Early intervention can help facilitate continued service of the tooth with predictable clinical outcomes. However, early intervention is not always possible and cuspal fractures are commonplace.
The assessment for structural compromise involves evaluating the current state of the tooth along with the characteristics of the existing restoration. Width and depth of the restoration are carefully considered, followed by the thickness of all cusps at their base. Careful evaluation of the inside of the tooth (dentin) with high magnification is done to identify any recurrent decay and possible crack propagation. Wide restorations and thin cusps are characteristic of a tooth that is structurally weak and in need of a stress-reduced direct composite restoration (SRDC) or a full coverage ceramic restoration.
In this case, the existing alloy is shallow but wide. The cusps are severely undermined, resulting in the loss of one cusp under normal function. Cracks can be seen propagating across the pulpal floor resulting in a dehydrated and brittle structurally compromised tooth. Traditionally, this cracked tooth would be planned for a full coverage crown resulting in the loss of roughly 75% of coronal tooth structure. A Master of Biomimetic Dentistry like Dr. Jihyon Kim, however, has the advanced clinical skills and material knowledge to restore this tooth esthetically and functionally while preserving both tooth structure and pulp vitality.

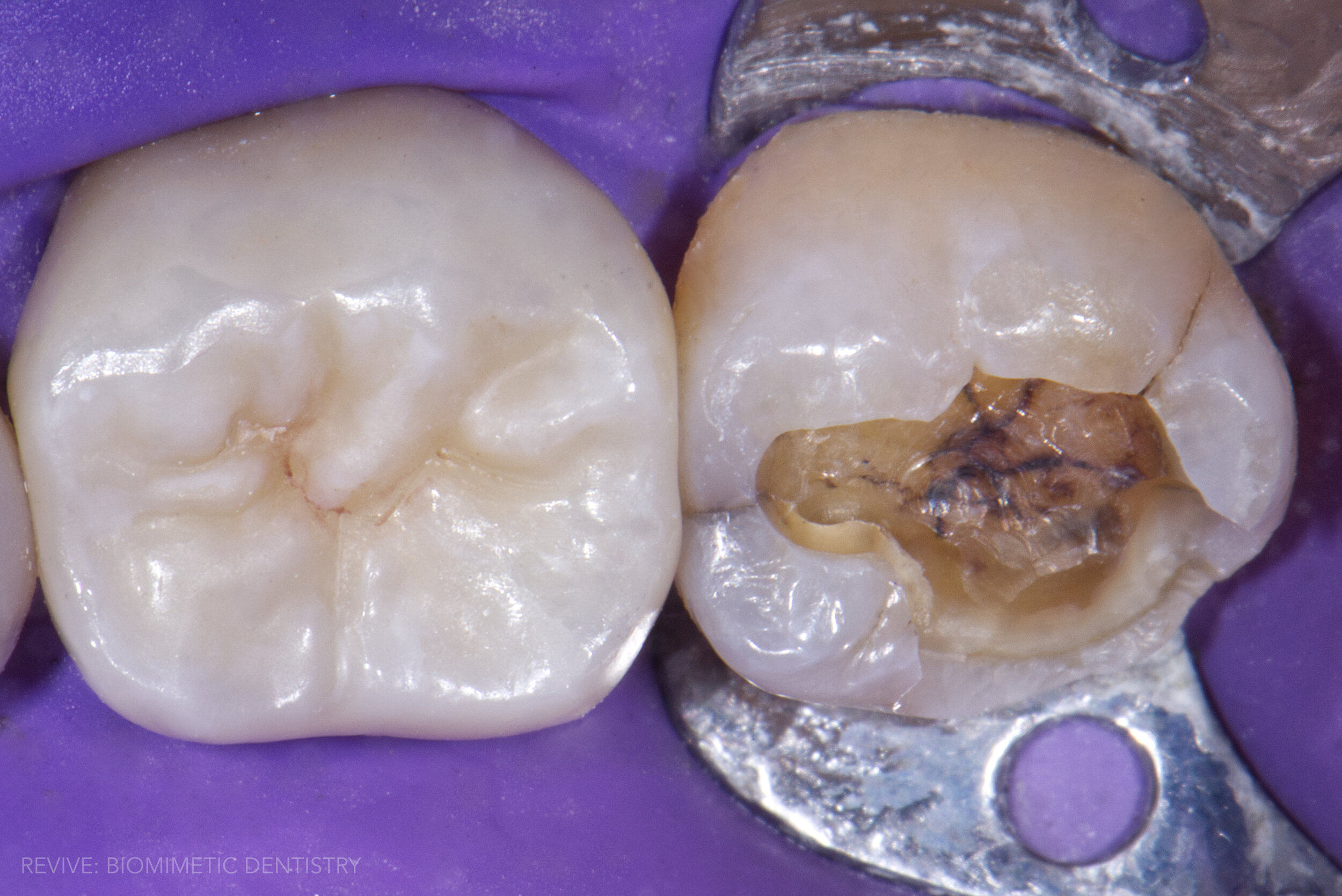
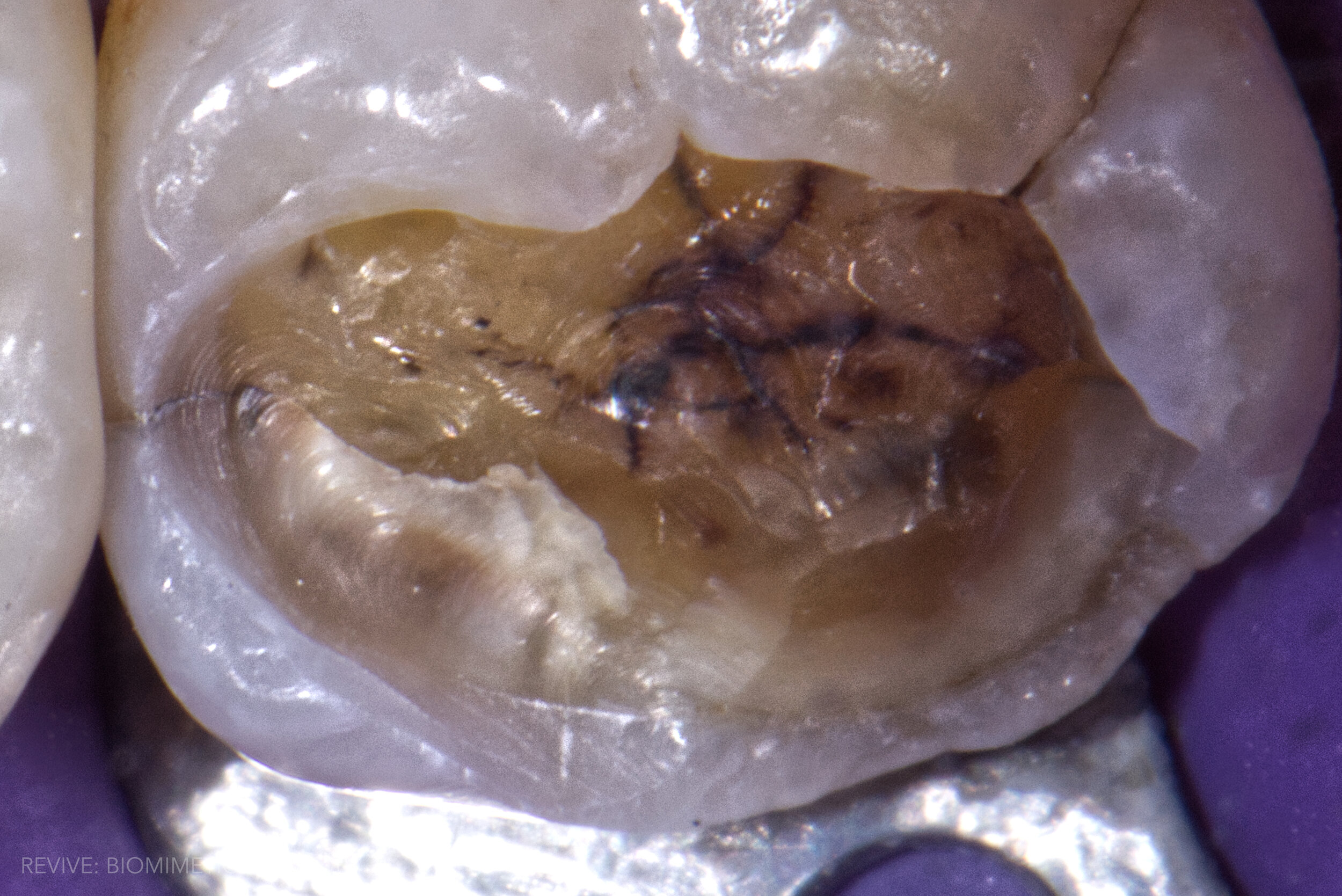



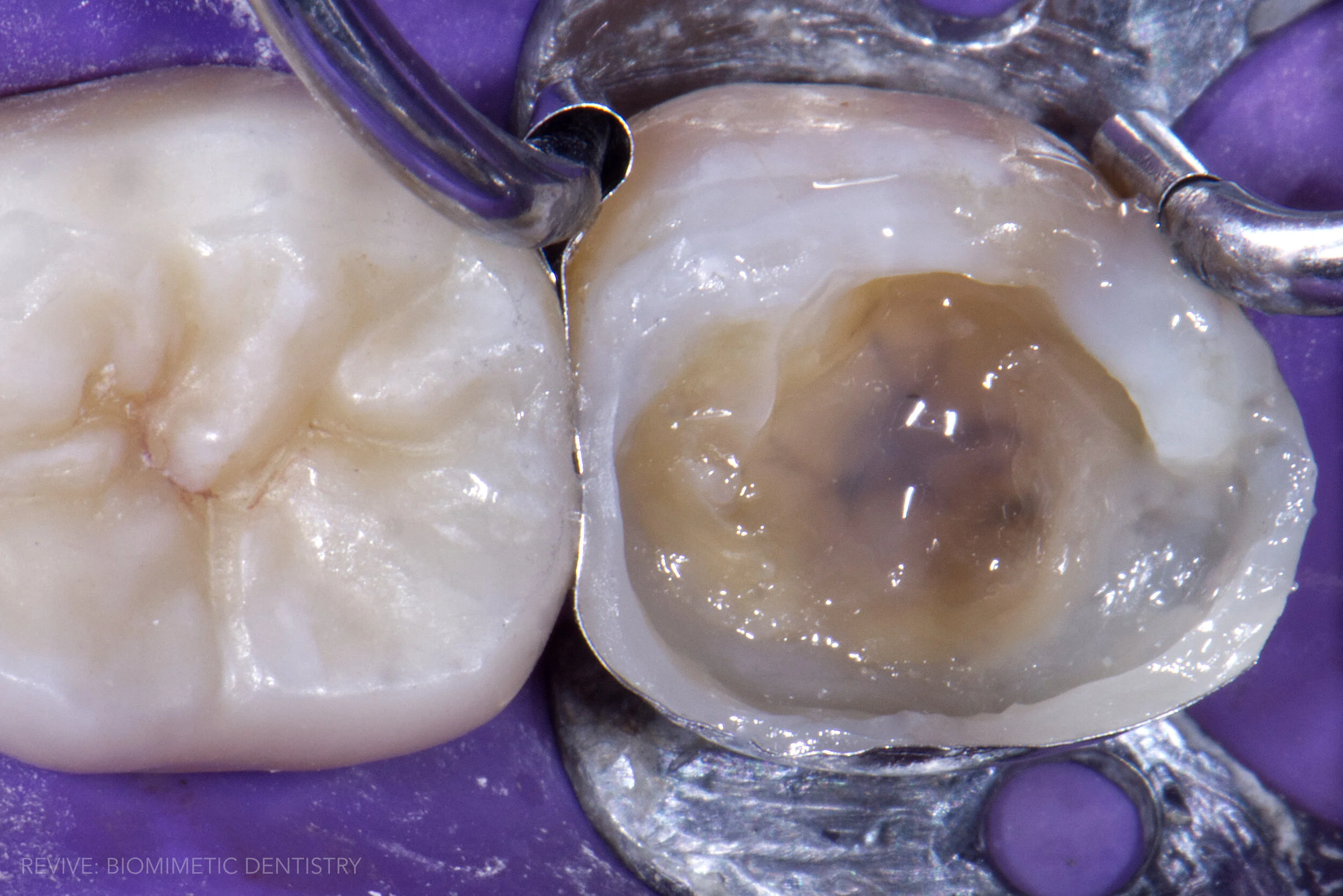


Our high-magnification surgical microscope and high-resolution clinical photography tell a story of a severely compromised second molar stricken with weak cusps and extensive dentin cracks. Crack dissection reveals dehydrated, disconnected dentin. Upon removal of the dehydrated dentin, continuation of the peripheral rim crack to the oblique crack can be fully appreciated. Left untreated, long-term prognosis for this tooth is poor, and a catastrophic crown/root fracture is likely.
Dr. Kim masterfully deconstructed and restored this case using the most advanced biomimetic protocols and materials on the market. Gold standard adhesive ClearFil SE Protect and Majesty Flow were used to seal the dentin and form a high-integrity bond layer, followed by AP-X and a 4x6mm section of Ribbond fiber, which serves to increase the bond strength of restorative material to the inside of the tooth while providing an artificial crack-stop with characteristics that closely mimic a natural tooth. The final enamel replacement layer is completed with warmed, monolithic and highly polished injection overmolded composite.
The patient can now appreciate the strength and longevity of this stress-reduced direct composite restoration for years to come. If you or someone you know may benefit from these conservative, tooth-saving techniques, we welcome you to contact us today for an honest consultation. If you have old, failing restorations or if you’ve been diagnosed with cracked tooth syndrome and told you need full coverage crowns, we would be happy to offer our expert input with a second opinion. We hope you enjoyed this case presentation.